
Ok, so you’ve been diagnosed with Hypothyroidism or Hashimoto’s thyroiditis, and you’re wondering about your hypothyroid treatment options.
Perhaps this just happened or maybe you’ve been living with and managing thyroid disease for years or even decades.
What do you do now?
If you’ve had hypothyroidism for years and feel like it’s well managed, you simply need to have a yearly blood check (review the full panel to ask for!) to make sure the medication(s) you are taking is still appropriate and doses don’t need to be adjusted.
If you’re new to this rodeo OR you have had hypothyroidism and are on medication but have never really felt any difference with the treatment you were prescribed, here we go:
What are my treatment options for hypothyroidism/Hashimoto’s?
Medication:
I don’t typically think of thyroid medication as first-step therapy unless a woman is trying to get pregnant or already pregnant or breastfeeding, but I know it’s by far the most common hypothyroid treatment option given so I wanted to discuss your options here first.
The medications available are all, with one exception, replacing the thyroid hormone your body is struggling to make.
Here’s how it works in the body:
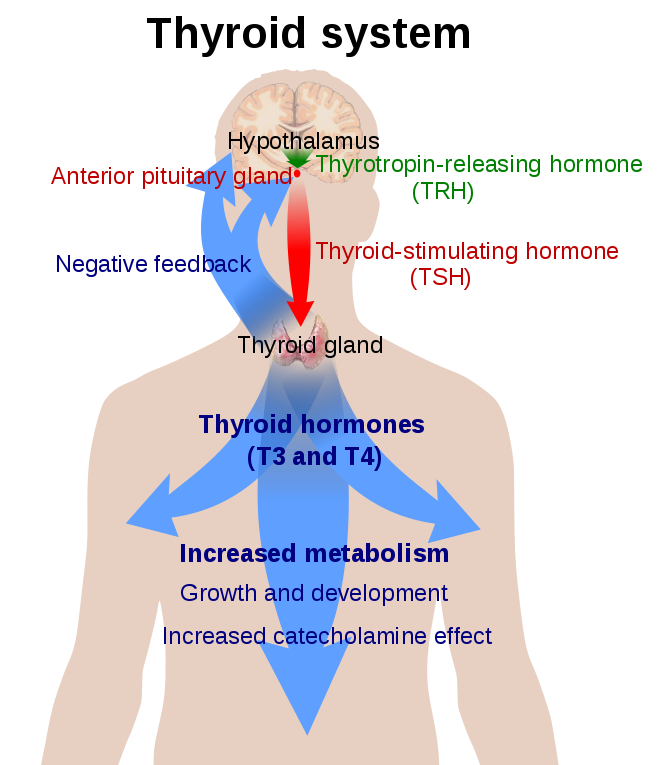
Your brain makes TSH (thyroid stimulating hormone) which, aptly named, stimulates the thyroid gland to make mostly T4 and a bit of T3. T4 is then circulated through the bloodstream where it is converted to T3 hormone.
While both hormones have big actions in the body, T3 hormone is the more active player. It’s important that your body has both.
Both T4 and T3 send signals back to the brain to either turn up the volume on TSH production (which translates to your body needing MORE medication) or to turn it down (which can mean you need LESS medication).
I like to think of TSH as a volume control. The HIGHER it is, the LOUDER your brain is having to communicate to your SLOW thyroid to make hormones. Your hormone production is SLOW or LOW when TSH is HIGH. And, the MORE thyroid hormone you make or take as medication, the LOWER the TSH will be. It can become too low, which tells your provider that you need LESS medication.
That can be confusing, but the summary is this:
- High TSH = low T4 and T3 hormones being made/taken
- Low TSH = high T4 and T3 hormones being made/taken
I think it’s important to understand the very basics of thyroid hormone production because it relates to your medication options, which are outlined below.
- Levothyroxine = Levothroid = Levoxyl = Synthroid = T4 hormone.
This is, by far, the most common thyroid medication prescribed. It is one of the most common meds prescribed in general, on many Top 5 lists for all pharmaceuticals together. When prescribed correctly and monitored well, it is an extremely safe medication.
Your body takes in the T4 hormone replacement and should convert it to T3 hormone.
Your body should then tell your brain to make less TSH.
You should see TSH levels come down to ideal values.
Your Free T4 and Free T3 lab values become ideal.
You should feel better!
- Liothyronine = Cytomel = T3 hormone
I don’t see Cytomel prescribed as frequently by my conventional primary care colleagues in the Seattle area, but I have noticed endocrinologists recommending this med occasionally, and I do as well.
Why? Some people’s bodies don’t convert T4 hormone to T3 hormone well.
These folks may be deficient in some nutrients (zinc, selenium) or genetically they may just not be efficient at it.
In these women, using T3 in addition to T4 allows the body to give the proper signals to the brain to lower TSH.
Subsequent lab checks for TSH, Free T4, and Free T3 should show ideal ranges, as previously discussed.
You should feel better!
Bummer: of all the hormone medication options, I see Cytomel (T3) being the most irritating to women’s bodies. Even when labs look good/normal/better, women frequently report heart palpitations and hair loss. I don’t use it much for these reasons. Many women do really well with the addition of Cytomel, I’m just always cautious about adding it.
In some practices, providers will use higher doses of Cytomel alone. This is called the Wilson’s Protocol. I don’t follow this protocol in my practice for the reasons I mentioned above.
- Nature-throid & Armour thyroid & NP thyroid = glandular thyroid
These are all medications containing both T4 and T3, sourced from pig thyroid glands.
Say what now? It’s true, these are pig gland medications. They are available at your conventional pharmacy.
Some people believe these are more natural because they come from an animal and are not made in a lab. I don’t think of this medication in this way. It’s still manufactured in a lab. It is still hormone replacement.
So, what’s the difference? The medication contains BOTH T4 and T3 in one pill. That can be great for minimizing the amount of medications you take per day. It also has slightly higher amounts of T3 than T4 and some bodies do really well with that. In my experience, women seem to tolerate the T3 in these gland therapies better than Cytomel.
Because all pigs are unique (just like us!), the amount of thyroid hormones in each batch of glandular medication varies. Some bodies do fine with that variability. Others really do not and we can see wild changes in lab results and patients report feeling over or understimulated from batch to batch. That is certainly not every woman’s experience, but it does happen.
I’ve noticed that all of these medication options are just that: OPTIONS for managing hypothyroidism and Hashimoto’s. I have not seen one-size-fits-all with any of these. I respectfully disagree with the providers that believe there is one medication that is best for all women with thyroid disease.
Because it’s the most simple and well-tolerated, I usually have women start Levothyroxine (T4). This allows us to not only see how she feels on the new medication but also to track how her body is converting the T4 to T3. If she needs T3, we can talk about Cytomel or a change to Armour or Nature-throid.
- Low-dose naltrexone (LDN)
LDN is a compounded medication that can decrease thyroid antibodies in Hashimoto’s thyroiditis (and perhaps in other autoimmune diseases). This drug must be prescribed by your provider and made at a special pharmacy in the ultra-low doses that are effective (1.5-4.5mg).
Naltrexone in its standard dose of 50mg (or more) is a medication that is used in helping people overcome alcohol and opiate addictions. It is an “opiate antagonist”, which means that it works by blocking the activation of opioid receptors. Instead of controlling withdrawal and cravings, it treats opioid & alcohol use disorder by preventing any opioid drug or alcohol from producing rewarding effects such as euphoria.
In smaller/lower doses of Naltrexone, the body’s endorphins are released. These endorphins have an effect on the immune system that decreases inflammation and the production of antibodies against the self. It’s pretty cool! I have a handful of patients managing their Hashimoto’s on this medication alone.
It can have uncomfortable side effects, so I don’t prescribe it often. Women report sleep disruption, nightmares, and headaches. I work with many perimenopausal and menopausal women who are already struggling with these symptoms and few are willing to potentially worsen that.
It can also cause nausea and worsen constipation or diarrhea.
LDN is typically started at 1.5mg and titrated up every 1-2 weeks by 1.5mg until the therapeutic dose of 4.5mg is reached.
Eating well
In my practice I see diet being less of an issue with pure hypothyroidism versus Hashimoto’s. That said, generally a healthy diet is the best course for any chronic disease management. What’s a healthy diet? I like Michael Pollen’s recommendation, “Eat real food. Not too much. Mostly Plants.”
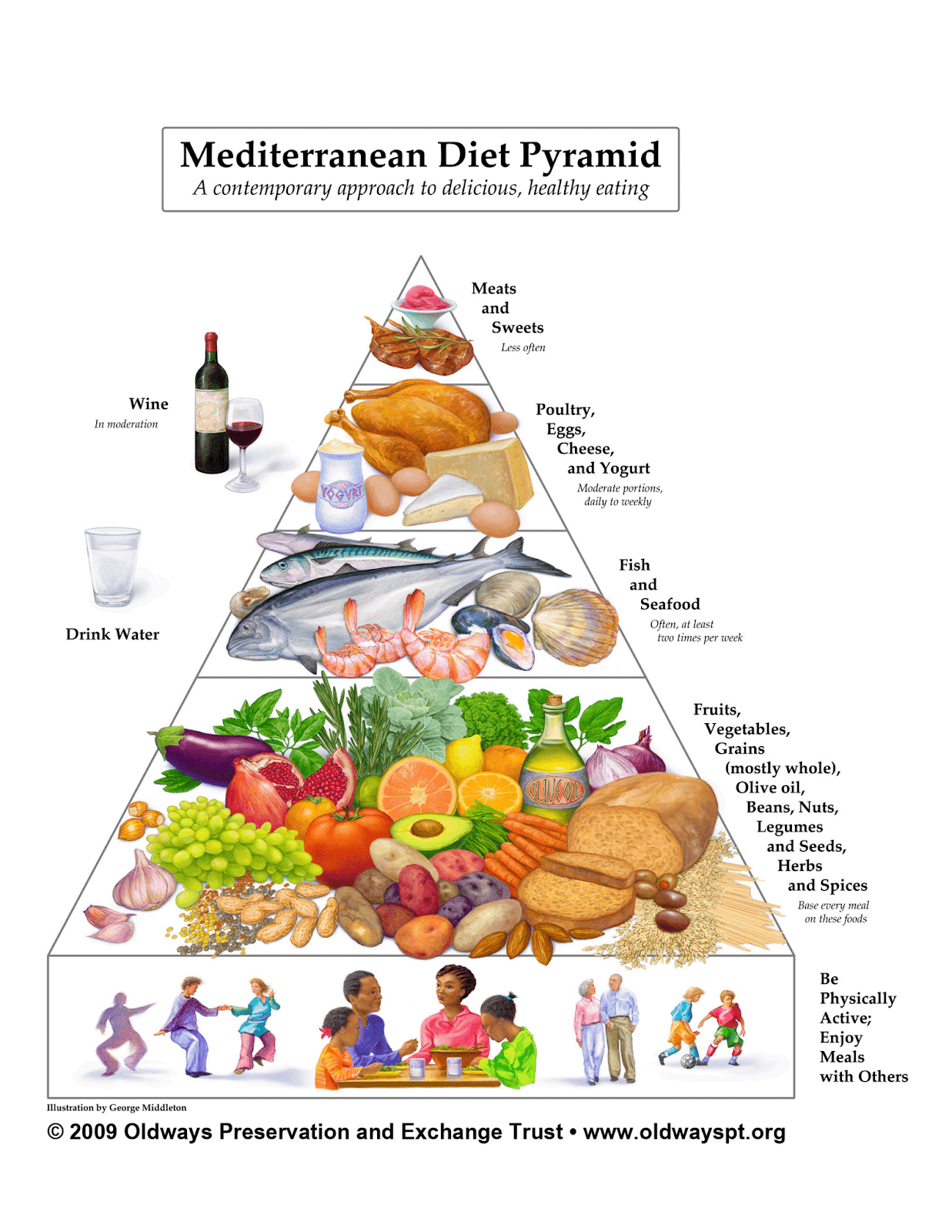
I am a fan of the Mediterranean Diet and appreciate the food pyramid associated with that style of eating.
With Hashimoto’s, driven by an inflammatory process in the body, I find it crucial to dig deeper. I frequently observe foods triggering inflammatory reactions in the body, and they may not always be the ones you suspect. I recommend following an anti-inflammatory diet approach like the Whole 30 or Autoimmune Paleo diets and then testing thyroid antibodies to check for changes. How long should you follow a diet like this? It varies per person, but I suggest at least a month, if not 2 to 3 months.
If these diets seem too extreme, start by addressing a common inflammatory culprit: gluten. As I mentioned in previous posts, if you have Hashimoto’s, your risk of Celiac disease—a severe autoimmune intestinal reaction to gluten—increases. Before you eliminate gluten from your diet, ask your provider to screen you for Celiac disease.
Managing your Stress
Managing any chronic disease or condition should include managing your stress levels. I encourage women to think about their stress. Perform a self-check on stress. On a scale of 1 – 10, how stressed are you now? If you are higher than a 5, I encourage you to change what you can. Sometimes people need to either lower the demands on themselves (say “no” more, end toxic friendships/relationships) OR experiment with different stress coping skills until they find ones that work for them.
Ideas:
- Deep breathing for 5 minutes
- Guided meditation for 5-10 minutes daily (apps I like: Calm, Shine, Insight Timer, Head Space)
- Put your devices away & observe what’s around you
- Play with your kids
- Take a date night with your partner
- Craft/draw/knit/sew/paint
- Relaxing (yin) yoga for 10-20 minutes
- Warm bubble bath with 10 drops of lavender essential oil
- Read fiction
- Take a walk outside
- Take a walk with friends
- Call a close friend or family member
Why is it important to keep stress in check? When your mind and physical body are stressed it creates a cascade of hormonal changes that can slow the thyroid down and worsen the autoimmune response. It can be much harder to manage your thyroid disease when stress is unregulated. Plus, when you’re less stressed, you’ll be more fun to be around!
Using Natural Therapies
- Nutrients
I encourage women to have their zinc, selenium, iron, and vitamin D tested. Supplement if needed to bring values into the high end of the normal range. If a woman is low in these nutrients, I delay adjusting medications until the nutrients have normalized. Frequently, thyroid hormone production improves when these nutrients are in ideal ranges.
If you have pure hypothyroidism (no Hashimoto’s antibodies are present), you need to avoid goitrogens. Goitrogens are foods that decrease thyroid hormone production by interfering with iodine uptake. When not enough iodine is available, the thyroid cannot produce sufficient levels of thyroid hormones T4 and T3. The brain senses the low T4 hormone and produces more TSH. The thyroid gland responds to TSH by making more hormones, but if it can’t keep up with demand, the thyroid grows. A swollen thyroid gland is called a goiter.
- Goitrogenic Foods:
- RAW Cruciferous vegetables: kale, cabbage, broccoli, turnips, Brussels sprouts, radishes, collard greens. NOTE: Cooking cruciferous veggies decreases goitrogenic content. **These are such a healthy veggie family that I encourage you to KEEP eating them, just cook them a little bit before enjoying them.
- Cassava, lima beans, sweet potato, sorghum, soy, millet
Interestingly, new studies show goitrogens are actually beneficial to those with Hashimoto’s thyroiditis by blocking iodine uptake. Lowering iodine levels lowers the antibody activity within the thyroid gland. Goitrogenic foods have also been found to increase levels of the antioxidant glutathione, which lowers oxidative stress in the gland to slow the rate of destruction of the thyroid cells.
- Iodine
This essential mineral is vital to proper thyroid hormone production. Your body needs small amounts for normal function, but many people are deficient. Your body can’t make iodine, so you must get it through your diet or supplementation. We lack robust tests for iodine deficiency, so I recommend women regularly incorporate iodine-containing foods into their diet.
These include:
- iodized salt, seasoning mixes with iodized salt, and onion salt or garlic salt made with iodized salt
- seaweed (kelp, nori, kombu, wakame)
- food additives: carrageen, iodides, alginates, iodate
- egg yolks
- most seafood except fresh-water fish
It’s important to get enough iodine but not too much. There are iodine-replacing protocols that use milligram (mg) doses of iodine when the body only needs around 200 MICROgrams (mcg). Mega doses of iodine can worsen hypothyroidism and autoimmune Hashimoto’s. Balance is key.
- Herbal therapy
Ashwagandha: This Ayurvedic stress adaptogenic herb has been shown in at least one study to increase triiodothyronine (T3) and thyroxine (T4) levels by 41.5% and 19.6%, respectively, and reduce serum TSH levels by 17.4% from baseline. That’s significant! The dose in the study was 600mg per day, and I usually recommend this dose. You can safely take up to 1000mg per day. BONUS: taking it at bedtime may improve sleep quality. DOUBLE BONUS: Ashwagandha is an adrenal hormone adaptogen. It normalizes your body’s response to the stress hormone, cortisol!
Avoid toxins
Increasingly research shows a correlation between common toxins in our environment and risk of disease. Hypothyroidism is one such condition. The chemicals we know affect the thyroid gland are:
- Flame retardants = organohalogens
- Furniture, some children’s clothing, children’s toys
- Alkylphenols
- Personal care products (shampoo, lotions, cosmetics), detergents, cleaning products, paints
- PFAs/PFCs = Poly- and perfluoroalkyl substances and perfluorinated compounds
- Found in textiles, food packaging, and firefighting foam
- Phthalates
- Personal care products (shampoo, lotions, cosmetics), food packaging, soft plastics, vinyl flooring, vinyl products, old toys
WOW. These chemicals are everywhere. What’s a gal to do? Do your best. Reduce your exposure to these chemicals. Use the Environmental Working Group’s wonderful catalog of databases to help you find safer options for you and your family:
- Skin Deep
- Choose products rated 0-2.
- I’m in LOVE with Beautycounter, a personal care product company whose mission is to “get safer products into the hands of everyone.” Try them at www.beautycounter.com/melissamccarty
- Guide to Avoiding PFAs
- Cleaner’s database
- Choose products rated A
- Home Guide
How often should I get tested?
When you first start your hypothyroid medication and each time you change the dose, you’ll want to get retested again in 6-8 weeks. This is the length of time it takes your body to assimilate the medication and for labs to change.
Once you’re on the best dose of medication or the best natural treatment regimen, you’ll want to get tested at least annually.
When it comes to hypothyroid treatment options, you have plenty of choices!
Have more questions about your hypothyroid treatment options? Want to work together to optimize your health and thyroid? Call or email the office and schedule a telemedicine visit. If you live in Washington state, your insurance may cover our visit!
Stay well!
Email me with questions: perimenopausenaturally@gmail.com
Follow me on Instagram: melissamccartyND
Like me on Facebook: Melissa McCarty, ND
